
Feeling Drained? Iron Deficiency Could Be Why

In previous posts, I've alluded to the fact that most of what I know about health has come from personal experience—from having to figure things out the hard way. A few weeks ago, I mentioned my protracted bout with SIBO (Small Intestinal Bacterial Overgrowth), but I didn't fully explain what came next: a cascade of nutritional deficiencies that quietly dismantled my health from the inside out. SIBO doesn't just cause uncomfortable digestive symptoms; it creates a perfect storm for malabsorption, as the bacterial overgrowth literally competes with your body for the vitamins and minerals it needs to function.
In my case, one of the most devastating consequences was iron deficiency—an unusual situation for a man, since we don't experience the regular iron loss that menstruating women do. At its lowest, my ferritin dropped to 26 ng/mL, which despite many doctors dismissing it as acceptable, is clinically classified as absolute iron deficiency. Suddenly the crushing fatigue, brain fog, heart palpitations, and dramatic hair thinning all made sense. My body had quietly entered iron rationing mode.
The frustrating part was that multiple doctors missed it entirely. "Your hemoglobin is normal," they'd say, and that was that. It wasn't until I requested ferritin testing myself—and fell down a rabbit hole of research on non-anemic iron deficiency—that I finally understood what was happening. Recovery has been slow, nearly two years of strategic supplementation, but the transformation in my energy, mental clarity, and overall wellbeing has been nothing short of remarkable.
What Exactly Is Ferritin? The Science You Need to Know
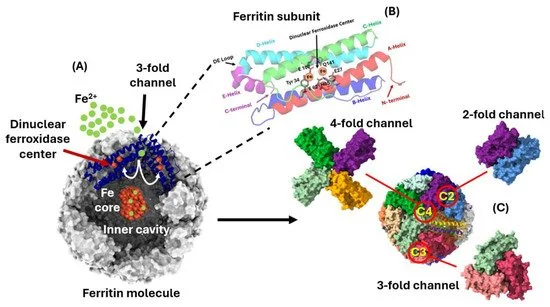
see Figure 1 in Arosio et al., 2025
Let's start with the basics. Iron is essential for over 180 different biochemical processes in the body, and it exists in several forms—primarily in red blood cells as hemoglobin, but also in muscle cells as myoglobin, and in storage compounds like ferritin and hemosiderin.
That last one is worth understanding, because ferritin is more than just a number on a lab test. When you consume iron, it circulates in your bloodstream as serum iron—but free-floating iron can actually be dangerous, so the body wraps any excess in a protein casing and tucks it away for safekeeping. That stored form is ferritin, and it functions as your body's iron reserve.
The key word there is reserve. When your iron intake is insufficient, your body begins drawing down those stores. As they deplete, it shifts into a kind of rationing mode—prioritizing which processes receive the limited supply. Critical functions, like delivering iron to bone marrow for red blood cell production, stay funded. Non-essential ones, like hair growth, get cut first. This is why you can experience all the hallmark symptoms of anemia—fatigue, brain fog, hair loss—well before you're technically anemic.
Several sources suggest that traditional lab reference ranges set ferritin thresholds too low to capture clinically meaningful iron deficiency. Breymann et al. found that women can experience symptoms at ferritin levels below 100 ng/mL—well above the commonly used treatment cutoff of 40 ng/mL. The same pattern holds in chronic inflammatory conditions: guidelines for heart failure, chronic kidney disease, and inflammatory bowel disease frequently define iron deficiency as ferritin below 100 ng/mL or transferrin saturation below 20%.
The Iron Panel: What All Those Numbers Mean
Your typical iron blood test includes several measurements that tell different parts of the story:
Serum Iron: The active iron currently circulating in your bloodstream
Transferrin: The protein that transports iron through your body
TIBC (Total Iron Binding Capacity): How much iron your transferrin can potentially bind
% Transferrin Saturation: The percentage of your transferrin currently carrying iron
Ferritin: Your iron storage reserves
When your body senses iron deficiency, it produces more transferrin (raising your TIBC) in a desperate attempt to capture any iron that comes in. This is why many iron-deficient people have high transferrin/TIBC but low % saturation.
Dr. Soppi's research highlights the profound, often overlooked impact of fatigue in non-anemic patients, drawing from extensive clinical observations. These patients—typically enduring diagnostic odysseys spanning years as inpatients and outpatients—suffer from debilitating exhaustion, rendering them unable to maintain employment or daily functions.
Key expansions from his work:
Diagnostic Challenges: Many undergo exhaustive testing without pinpointing the cause, leading to misdiagnoses like chronic fatigue syndrome or depression. Soppi notes this fatigue stems from subtle metabolic or inflammatory disruptions, not always captured by standard anemia screens.
Functional Impairment: Extreme tiredness mimics severe illness; patients report inability to work, with some bedridden for days. Quality-of-life metrics plummet—Soppi likens it to "close to zero," akin to end-stage chronic disease.
Economic Burden: Healthcare costs skyrocket from prolonged evaluations (e.g., repeated hospitalizations, specialist fees), while lost productivity adds indirect expenses.
Iron 101: Heme vs. Non-Heme
Iron comes in two forms, and they're not created equal:
Heme Iron: Found in animal products (red meat, poultry, fish). Your body absorbs this easily—about 35%. For readers looking for a heme-based option, Three Arrows Iron Repair provides 20 mg of elemental iron per serving from concentrated bovine spleen. It’s the one I preferred using.
Non-Heme Iron: Found in plants and most supplements. Absorption rates? A measly 2-20%. This needs vitamin C as a wingman to be properly absorbed.
Calculating Your Iron Needs
For those dealing with iron deficiency, medical research points to the following daily intake targets based on body weight:
Minimum daily intake (non-heme iron): weight in kg × 2 mg
Maximum daily intake (non-heme iron): weight in kg × 5 mg, capped at 400 mg
Minimum daily intake (heme iron): weight in kg × 1.5 mg
Maximum daily intake (heme iron): weight in kg × 2 mg
The 400 mg ceiling on non-heme iron isn't arbitrary—beyond that point, transferrin becomes saturated and can no longer safely transport additional iron through the body.
The Surprising Causes of Low Ferritin
Iron deficiency has more entry points than most people realize. Here's a breakdown of the most common culprits:
Blood Loss and Increased Demand
Heavy periods (the leading cause in women)
Pregnancy and breastfeeding
Endometrial polyps and fibroids
Miscarriage and childbirth blood loss
Absorption Issues
Low stomach acid, often worsened by antacids
SIBO or H. pylori infection, which compete directly with the body for iron
Hypothyroidism, which affects iron metabolism
Celiac or Crohn's disease
Post-bariatric surgery, which removes portions of the gut involved in iron absorption
Medications like proton pump inhibitors
Diet and Timing
Vegan and vegetarian diets, which contain no heme iron
Taking iron alongside calcium or coffee, which significantly inhibits absorption
Appetite suppressants that reduce overall nutrient intake
Bleeding
Regular blood donation
Bleeding disorders such as hemophilia
Gastrointestinal bleeding from ulcers, NSAID use, or cancer
Hookworm infections causing chronic blood loss
Iron Depletion
Bacterial or parasitic competition for iron
High-dose supplements that interfere with iron metabolism
Compounds like turmeric, curcumin, and quercetin, which may chelate iron
Hyperoxaluria, where elevated oxalate levels bind to iron
Rare Causes
Genetic mutations affecting iron metabolism
Premature birth leading to nutritional deficiencies
Nutritional deficiencies during pregnancy affecting fetal iron stores
What You Need to Know About Labs
One reason iron deficiency goes undiagnosed so often is that most doctors rely on a standard iron panel rather than testing ferritin directly. Here's what the numbers actually mean:
Ferritin is your iron storage protein and the single most specific indicator of true iron status
Below 30 µg/L: Absolute iron deficiency, confirmed by multiple peer-reviewed studies
Below 100 ng/mL: Clinically significant symptoms can occur even without anemia
Target range: Research suggests at least 125 ng/mL, and up to 200 ng/mL for those who have been deficient for an extended period
Measuring serum iron alone is like counting the cash in your wallet on payday; it tells you only what's immediately available, fluctuating with every meal. Ferritin, by contrast, is like the money in your bank account. It represents your body's accumulated savings: the iron stored across tissues and organs over months. Normal serum iron can coexist with a dangerously depleted ferritin reserve, which is exactly why the diagnosis gets missed.
The Path Forward
If you suspect iron deficiency, push for ferritin testing specifically—a standard iron panel won't tell you what you need to know. Research consistently shows that hemoglobin can appear completely normal while ferritin is critically depleted.
Recovery is rarely quick. Depending on how depleted your stores are, it can take months or years for your body to fully rebuild. But with the right approach and consistent follow-through, the improvement in how you feel can be profound.
Note: This post contains affiliate links, which means I may earn a small commission if you purchase through my link, at no additional cost to you. I only share products that are relevant to the topic and that I’ve personally found useful. Always make supplement decisions based on your own labs and guidance from a qualified clinician.
References
Arosio P, Cairo G, Bou-Abdallah F. A brief history of ferritin, an ancient and versatile protein. Int J Mol Sci. 2025;26(1):206. doi:10.3390/ijms26010206.
Breymann C, Römer T, Dudenhausen JW. Treatment of iron deficiency in women. Geburtshilfe Frauenheilkd. 2013;73(3):256-261. doi:10.1055/s-0032-1328271.
Dignass A, Farrag K, Stein J. Limitations of serum ferritin in diagnosing iron deficiency in inflammatory conditions. Int J Chronic Dis. 2018;2018:9394060. doi:10.1155/2018/9394060.
Peyrin-Biroulet L, Williet N, Cacoub P. Guidelines on the diagnosis and treatment of iron deficiency across indications: a systematic review. Am J Clin Nutr. 2015;102(6):1585-1594. doi:10.3945/ajcn.114.103366.
Soppi ET. Iron deficiency without anemia: a clinical challenge. Clin Case Rep. 2018;6(6):1082-1086. doi:10.1002/ccr3.1529.
Goodnough LT, Nemeth E, Ganz T. Detection, evaluation, and management of iron-restricted erythropoiesis. Blood. 2010;116(23):4754-4761. doi:10.1182/blood-2010-05-286260.
Camaschella C. Iron-deficiency anemia. N Engl J Med. 2015;372(19):1832-1843. doi:10.1056/NEJMra1401038.
López A, Cacoub P, Macdougall IC, Peyrin-Biroulet L. Iron deficiency anaemia. Lancet. 2016;387(10021):907-916. doi:10.1016/S0140-6736(15)60865-0.
Umbreit J. Iron deficiency: a concise review. Am J Hematol. 2005;78(3):225-231. doi:10.1002/ajh.20249.
Lynch S, Pfeiffer CM, Georgieff MK, Brittenham G, Fairweather-Tait S, Hurrell RF, et al. Biomarkers of nutrition for development (BOND)-iron review. J Nutr. 2018;148(suppl_1):1001S-1067S. doi:10.1093/jn/nxx036.
Kumar A, Sharma E, Marley A, Samaan MA, Brookes MJ. Iron deficiency anaemia: pathophysiology, assessment, practical management. BMJ Open Gastroenterol. 2022;9(1):e000759. doi:10.1136/bmjgast-2021-000759.